
Facies Midline

Please click to enlarge.
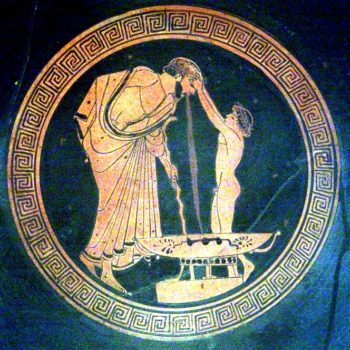
Note what signs you see.
I (I. Lastivka, M.D.) see facial midline dysmorphic signs. The clinical question is if these are signals of a syndrome.
PERSPECTIVE: The forebrain, during early embryogenesis evolves into lateral frontal lobes and a rhinoencephalon. These developmental fields impact the morphology of the facial midline. In this infant there is no evidence of supra-orbital prominence (“pseudo-shallow” orbits); the nasal bridge is virtually absent; the palpebral fissures are slanted upward; the midline and tip of the nose are underdeveloped; the upper lip filtrum is not developed; the vermilion of the upper lip is absent and there is no Cupid Bow – like outline of the vermilion-cutaneous junction of the upper lip. This cluster if dysmorphic signs signal that this face can be called a facies suggestive of holoprosencephaly.
We do not know anything else about this patient except what we have seen in the illustrated photograph. Therefore, to this point we have not been biased by interpretations of the referring clinician or his consultants. For the same reason we refused to look at laboratory or imaging study results until we examine all the visual materials illustrative of the morphogenesis of the patient.
Now we will read the clinical record which states or fails to state: the patient is 3 weeks old of “Gypsy” ethnic origin, perhaps from consanguineous parents (such assertion must be clarified or else should be considered dubious – it may reflect cultural bias of the clinician – many assume that being “Gypsy” implies parental consanguinity); amazingly no further information of the original clinical examinations is given. Instead the referring physician immediately jumps into “borrowed cerebral territory” of consultants who inherently know less about the patient than the referring clinician – they may know much about their specialty but not about the patient – otherwise the referring clinician should transfer the patient to the care of the specialists.
This is a classic example of the crisis of medical clinical arts – increasingly clinicians feel insecure about clinical examinations and seek help by chasing laboratory or imaging results and opinions of specialists who know little about the circumstances of the patient. Such fragmentation of clinical care is particularly dangerous for infants.
The rest of the consultation note summarizes what a radiologist and surgeon “said”, in other words, their opinions and not what they observed. Apparently the patient has signs of destructive processes in the left and right areas of tibio-tarsal ossification centers, and bilateral “afebrile abscess” (I doubt the accuracy of these statements).